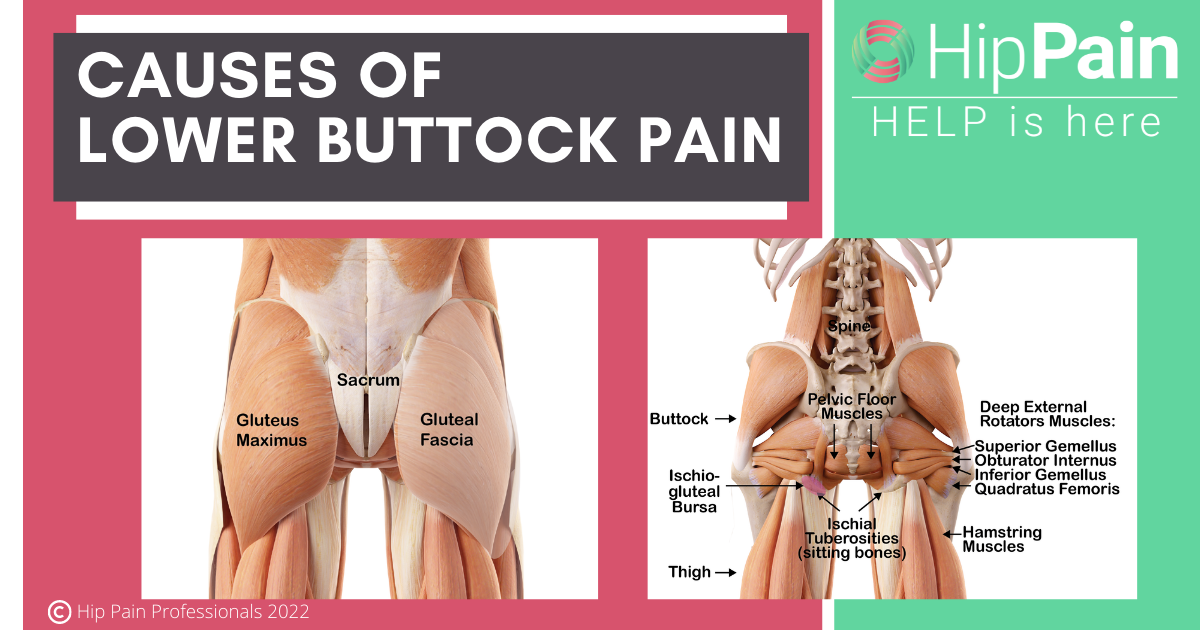
Have you heard of Botox injections for piriformis syndrome? Piriformis syndrome is one of several causes of irritation of the sciatic nerve as it runs through the buttock and down into the leg. This can result in sciatica – pain, tingling and various other nerve symptoms in the buttock and leg.
Buttock pain related to piriformis syndrome can have a profound impact on work, socialisation and quality of life due to symptoms experienced in sitting, and during and after physical activity.
Correct diagnosis is often delayed and effective treatments for piriformis syndrome can be difficult to access. Botox injections for piriformis syndrome are an option that might be explored if more traditional treatments have not been effective.
As physiotherapists (physical therapists) with over 50 years of combined experience with this condition, we’ll be sharing information from scientific research and our wide experience helping patients suffering from piriformis syndrome.

Recovering from Piriformis Syndrome, Deep Gluteal Syndrome or Hip Related Sciatica
FIRST LESSON IS FREE!
In this blog, we’ll take a close look at Botox injections for piriformis syndrome, covering the following main topics:
Piriformis syndrome has had a rocky ride as a diagnosis, because of its frequent incorrect use for pretty much any pain in the upper buttock. The word ‘syndrome’ also simply means ‘a collection of symptoms’, so it can be a bit non-specific as a diagnosis.
The diagnosis ‘Piriformis Syndrome’ should be reserved for situations where symptoms are known to be related to the sciatic nerve, and the underlying problem is irritation of that nerve by the piriformis muscle.
Broader terms such as Deep Gluteal Syndrome or Hip Related Sciatica may be used where the source of the sciatic nerve irritation is known to be at the hip (rather than the lower back). These broader terms are often used now because there are several locations at the back of the hip where the nerve may be irritated – including, but not limited to under or within the piriformis.
You can read more about piriformis syndrome and other causes of sciatic nerve irritation in the buttock by clicking on the coloured text in this sentence. You can also learn much more about these situations and what can be done to help in our self-help course for piriformis syndrome, deep gluteal syndrome and hip-related sciatica.


If you have pain deep in your buttock, which might extend down the back of your leg and to your foot, you may have this condition.
We have prepared a self-test in the first FREE LESSON of our self-help course.
You can find it here:
The main symptom of piriformis syndrome is deep buttock pain, that may extend down the back of the leg and even to the foot. There may be other nerve signs such as tingling, buzzing, zings and zaps and even numbness or altered sensation in the buttock or leg. Read more about symptoms of piriformis syndrome and hip related sciatica by clicking the coloured text in this sentence.
The diagnosis of piriformis syndrome can be challenging, leading to delays in both diagnosis and provision of appropriate and effective treatment. Because irritation of the nerve roots in the lower back is the most common cause of pain that radiates from the buttock down into the leg, investigation of the lumbar spine is usually undertaken first.
To complicate matters further, people with primary piriformis syndrome may end up with secondary or associated pain in the lower back. Many people with piriformis syndrome may then end up having treatments aimed at the lower back that do not help or only provide partial relief.
The first step then, in the effective management of piriformis syndrome, is getting the diagnosis right.
If you’d like to do a FREE SELF-TEST FOR PIRIFORMIS SYNDROME, to see if you may have this condition, head to our self-help course where the first FREE lesson helps you test yourself for piriformis syndrome or deep gluteal syndrome (sciatic nerve irritation in the buttock).
Once you have a diagnosis, the next challenge is seeking out the best treatment for piriformis syndrome. You can read more about the range of treatment options for piriformis syndrome by clicking on the coloured text in this sentence. Below, we will focus on the possible role of Botox injections for piriformis syndrome.
Botox or botulinum toxin is a neurotoxin produced by the bacterium Clostridium botulinum. This is the same toxin that causes ‘botulism’, a very dangerous form of food poisoning. A neurotoxin is something that is toxic to the nervous system. In this case, botulinum toxin causes paralysis of local muscles it is injected into, by preventing transfer of nerve impulses from the nerve to the muscle.
Doctors have found medical and cosmetic uses for this toxin, injecting very small amounts to achieve the desired results. You might be most aware of Botox as a cosmetic treatment, where it is used to paralyse muscles of the face, around the eyes and between the eyebrows, to reduce the appearance of wrinkles.
Botox is used in those with spasticity related to neurological conditions such as cerebral palsy or after a stroke. It has also been increasingly used to reduce muscle overactivity and pain in musculoskeletal conditions, such as piriformis syndrome.
Partial muscle paralysis may reduce pain from the muscle itself, and from other structures it might be squeezing, such as a nerve. Botox may also block the release of some neuro-peptides (amino acids) involved in the pain experience.


Recovering from Piriformis Syndrome, Deep Gluteal Syndrome or Hip Related Sciatica
FIRST LESSON IS FREE!
Botox injections have been used increasingly for those with piriformis syndrome – piriformis related irritation of the sciatic nerve.
A 2013 study by Michel and colleagues reported on a large case series of 121 patients who underwent Botox treatment for piriformis syndrome, after having a poor response to treatment with medication, massage and stretching.1
Of those who had one or more Botox injections, 77% reported good or very good improvements in pain levels, 7.4% average outcomes and 15.6% poor outcomes. While these sound like good outcomes, we need to be cautious of these results because this is not a rigorous study design. Randomised clinical trials reduce potential ‘bias’ or misunderstanding of the results and better clarify the usefulness of Botox.
In 2022, Elsawy and his research team published a randomised clinical trial which included a comparison of the effects of local anaesthetic injection against botulinum toxin injection for piriformis syndrome.2 The group of patients included, was once again, a group who had not received enough relief from standard medication and rehabilitation.
At one month after the injection, pain and function were significantly better for those who had the local anaesthetic injection, compared to those who had the Botox injection into the piriformis muscle.
However, 2-3 months after injection, the benefits of the local anaesthetic injection were reducing and the improvements in the Botox injection group were increasing. At 6 months, pain and function for those who had the Botox injection were significantly better than those who had the local anaesthetic injection.
These researchers concluded that Botox might help reduce pain and improve function in those with piriformis syndrome, in the medium to longer-term (>6 months). Local anaesthetic injection is more effective in the short term, for people who have not responded to physiotherapy (physical therapy) and medications.
Not yet tried a course of rehabilitation? Check out our self help rehabilitation course “Recovering from Piriformis Syndrome, Deep Gluteal Syndrome or Hip Related Sciatica”. Lesson 1 is completely FREE.


Botulinum toxin is a powerful neurotoxin, so great care must be taken when injecting such a substance into a human being. As the piriformis muscle is deep in the buttock, image guidance (using ultrasound or computerised tomography) is essential, to ensure the Botox is placed accurately within this muscle.
With accurate placement of the injection, side effects are mild and the procedure is considered safe.4,5 Mild local effects may include local discomfort and/or bruising at the injection site, local infection or allergic reaction. Other uncommon side effects including flu-like symptoms, temporary numbness, blurred vision, gastro-oesophageal reflux, constipation, and a wobbly neck have been reported in studies investigating the effects of Botox injection, all resolving without treatment 4,5
However, there is the possibility of other side effects related to the spread of the toxin into neighbouring structures or due to accidental injection into adjacent muscles, nerves or blood vessels.
Botox can spread 30–45 mm (1-2 inches) from the injected muscles, so injection into the piriformis could potentially spread to the adjacent gluteal muscles, or these muscles could be accidentally injected if adequate imaging is not used to place the needle tip. This would result in gluteal weakness.
Accidental injection of Botox into the bloodstream may result in generalised muscle weakness and fatigue for weeks or months, as the toxin is a muscle paralysing agent. In more severe cases, for example, if the whole dose was injected into the bloodstream, this situation could be life-threatening.5
Accidental injection into a nerve may result in loss of nerve function and therefore function of the muscles served by that nerve. The sciatic nerve is closely associated with the piriformis (which is why it may cause sciatic symptoms), so injection into the piriformis needs to be closely guided to avoid injecting the sciatic nerve. There are no reports of sciatic nerve injection in the literature, but this is a potential risk.
As with any foreign substance injected into the body, there is also always a very small chance of a systemic allergic reaction and anaphylaxis.5


Our advice, as physiotherapists (physical therapists) with wide experience with piriformis syndrome would be:
Recovering from Piriformis Syndrome, Deep Gluteal Syndrome or Hip Related Sciatica
FIRST LESSON IS FREE!
If you'd like a physiotherapist/physical therapist that knows hips to guide you through a recovery program, you can find the location of our Hip Pain Professionals below.
Visit our Pain Locator Map to learn more about pain in different regions around the hip and pelvis.
Top Tips for Hip Pain Relief Sitting, when Socialising or Travelling
Top Tips on Hip Pain Relief Sleeping
3 Simple Strategies to Reduce Hip Pain with Walking and Running
This blog was written by Dr Alison Grimaldi, an expert physiotherapist, educator and researcher with over 30 years working in the field, a special interest in the hip and 20+ years contributing to hip research.

Dr. Alison Grimaldi BPhty, MPhty(Sports), PhD is Practice Principal of PhysioTec Physiotherapy Clinic in Brisbane, an Australian Sports Physiotherapist, an Adjunct Senior Research Fellow at the University of Queensland, and a Fellow of the Australian College of Physiotherapists.
References