Many of you experience “hip flexor pain”. Your hip flexor pain might be felt with squatting, sitting, walking, running, climbing stairs, or cycling to name just a few activities people struggle with. Are you doing the best exercises to help your hip flexor pain? Or are some of your go-to exercises or hip flexor stretches contributing to your hip flexor pain, rather than helping it? And are you sure that the pain at the front of your hip is even hip flexor pain? This diagnosis is unfortunately grossly overused.
In this blog, we’ll be busting some myths and bringing you a range of information to help you better understand hip flexor pain and the causes and strategies for reducing hip flexor pain in common situations.
Here’s what we’ll be covering in this blog:
There are many reasons that going up stairs may result in more hip pain than other activities. Below we’ve outlined some of the common causes of hip pain walking up stairs.
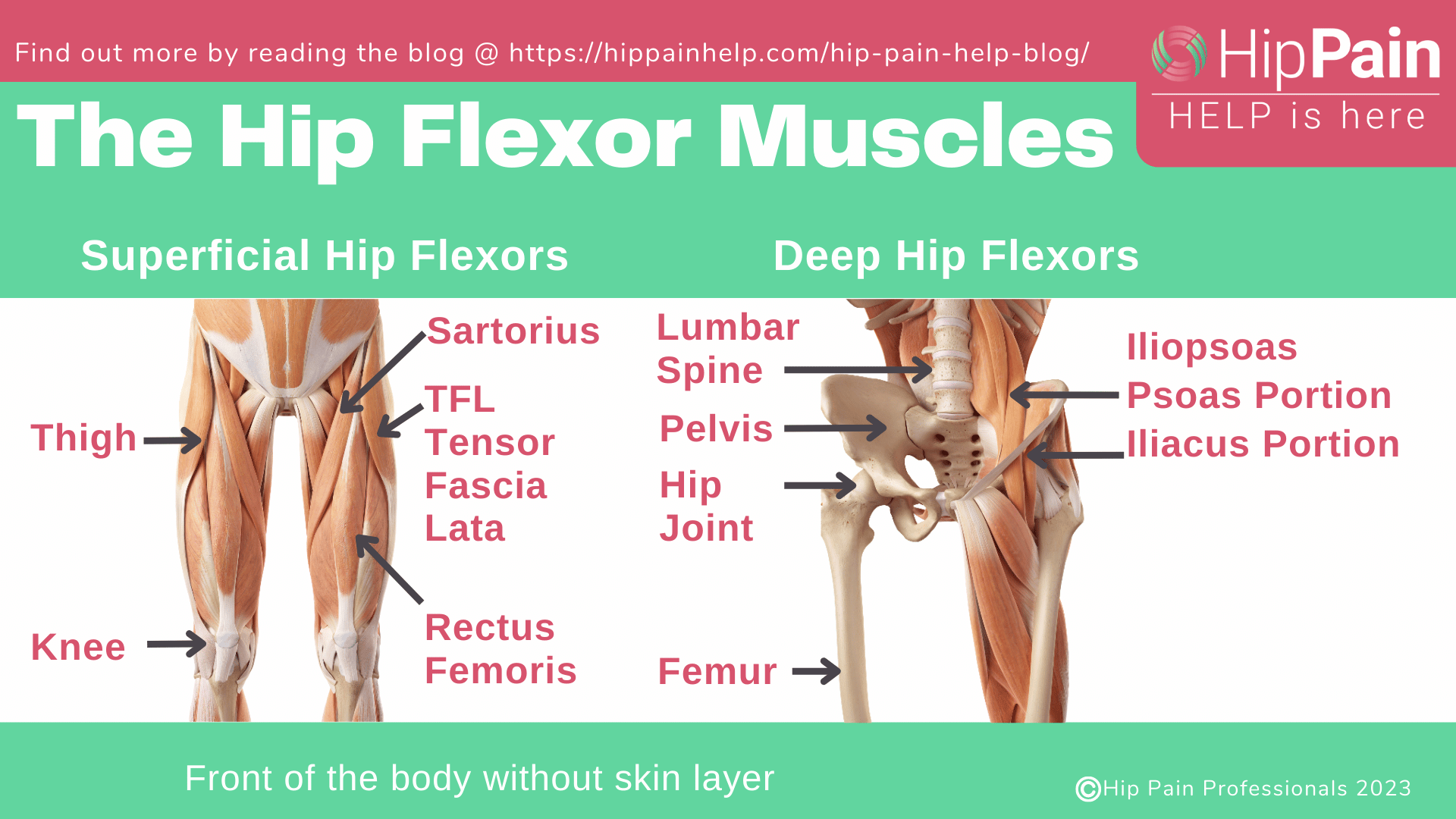
The hip flexor muscles are a group of muscles at the front of the hip, that help to ‘flex’ or bend the hip – lift the knee towards the chest. The main hip flexor muscle is the iliopsoas muscle. This is in fact 2 muscles – the psoas muscle and the iliacus muscle. These muscles are also important in supporting the femoral head (top of the thigh bone) in the socket bone (the acetabulum). The other muscles in the hip flexor complex include the rectus femoris muscle which also helps to straighten the knee, the sartorius muscle and the TFL (tensor fascia lata muscle). The iliopsoas also has a bursa, a small fluid filled sac called the iliopsoas bursa – this may at times also be irritated, known as bursitis. You can see the anatomy of the hip in the graphic below.
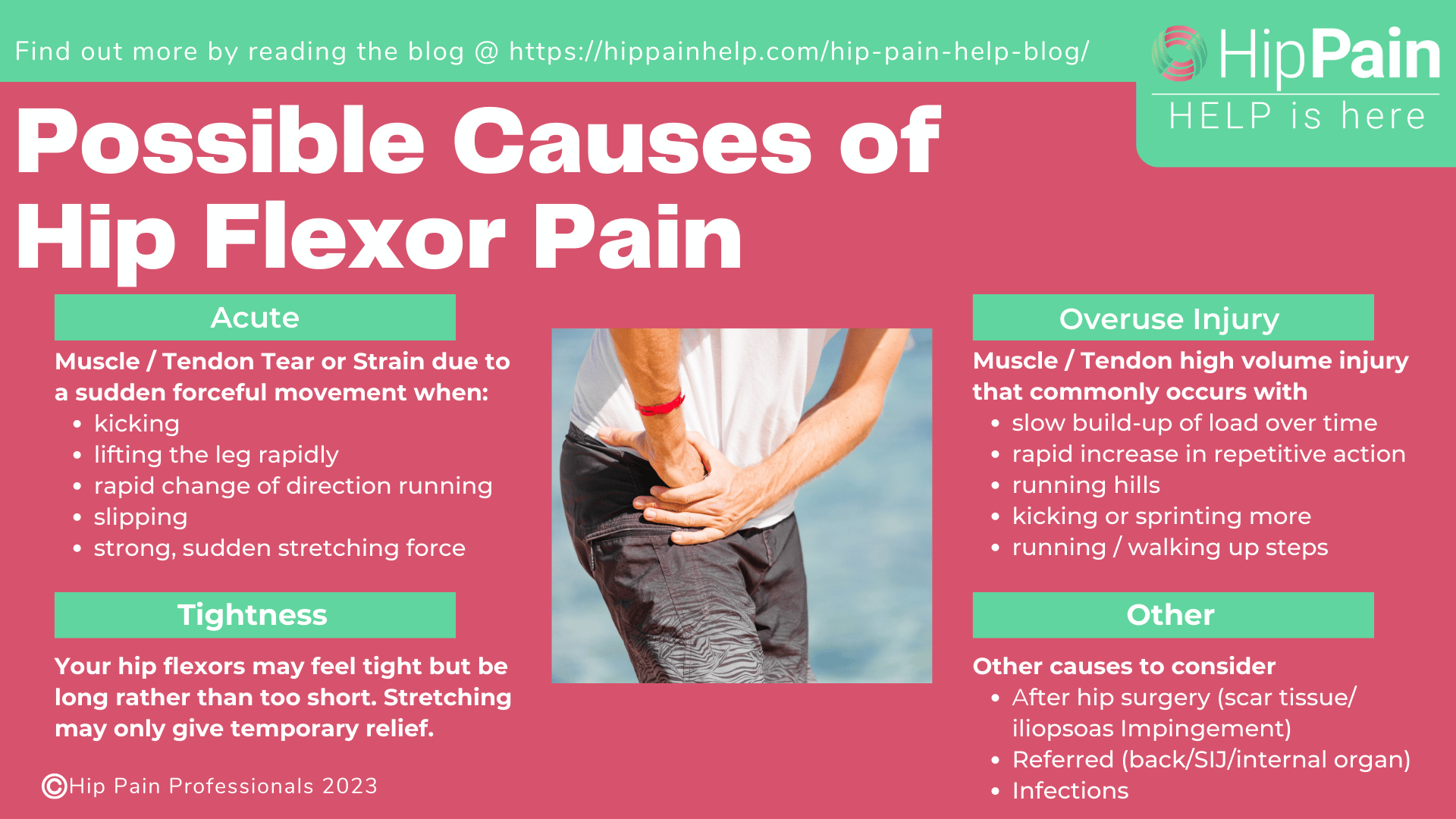
Hip flexor pain most commonly develops at the front of the hip (in the hip flexor area – anterior hip pain) after a sudden forceful action (acute injury), or not being able to cope with repetitive work over time, or during a rapid increase in workload (overuse injury). Another common belief is that hip flexor pain is related to hip flexor tightness and overactivity. Hip flexor pain may also develop after surgery.
The hip flexor muscles may be damaged due to a hip flexor tear or hip flexor strain. Hip flexor injuries usually occur with a sudden forceful movement such as kicking or lifting the leg rapidly, slipping, or a strong, sudden stretching force.
Acute hip flexor tears will be felt as an immediate sharp pain at the front of the hip – this might be quite severe pain at the time of injury. This might be accompanied by loss of function resulting in limping and difficulty stair climbing and lifting the leg to dress, or into a car or bed.
Alternatively, a minor tear where only a small number of muscle fibers are affected may quickly settle to a dull ache at the front of the hip, and the top of the front of your thigh. A feeling of tightness may be felt during daily activities such as rising from sitting, walking, or running with a long stride. This usually warms up with activity.
A strain of the hip flexor muscle usually occurs during strenuous activity. Hip flexor tears in field sport athletes, like football players or soccer players, have been shown to occur most commonly during a rapid change of direction when running.1 Hockey players and other running athletes, particularly those involving sprinting, and others participating in martial arts may also sustain this type of injury and develop a painful hip.
At times the tendons that join the muscles to the bone may be irritated either from a sudden movement, similar to a muscle strain.
The hip flexor muscles and tendons are also often affected by a slow build-up of load over time, or a rapid increase in a repetitive action. Pain related to high volume activity, rather than a single event, is often called an overuse injury.
This may follow a change in load, for example – doing more, doing something that is harder work, or doing a task that requires these muscles specifically to work more, for example, running hills, kicking more, sprinting more, or running or simply walking up more steps. Irritation to the tendons is known as tendinopathy or tendinitis.
A small bursa or fluid filled sack sits under the tendons at the front of the hip and may also become irritated for the same reasons. This is known as iliopsoas bursitis.
The hip flexor muscles are often incorrectly assumed to be tight or overactive. Tight muscles with reduced hip extension range of motion are often cited as the cause of not only hip flexor pain but all sorts of problems around the body.
Of course, some people have tight hips, but people with long hip flexors seem to have just as much trouble with pain at the front of the hip as those with tight hip flexors. We can’t just assume the problem is always tight hip flexors – often weak muscles might be the reason for sore hip flexors, and strengthening exercises may be much more helpful than stretching.
Hip flexor pain may also develop after hip surgery, such as after a hip arthroscopy or hip replacement surgery. This might be related to scar tissue, or impingement of the iliopsoas (hip flexor) tendon against the prosthesis after hip replacement.
Pain in the hip flexor region at the front of the hip can also be referred from the low back (lumbar spine), the pelvic joints (Sacroiliac joints or SIJ’s), or the internal organs. Occasionally the problem can also be an infection in the iliopsoas bursa, although this is not common.
The poor hip flexors are regularly subjected to strong stretching techniques, deep massage, trigger point release (often very painful), acupuncture, needling or cortisone injections, foam roller massage, and all sorts of other torture inflicted with a whole range of tools!
And how much evidence is there that any of these things help?? … Zip! Zero! None!
In fact, not only are most of these things a waste of time and money for ‘hip flexor pain’, not to mention very painful, some may make it worse, and the pain might not even be related to the hip flexors!
Many people are stretching their hip flexors and placing high loads on the front of the hip unnecessarily, often aggravating their symptoms.
Hip flexor pain may also develop after hip surgery, such as after a hip arthroscopy or hip replacement surgery. This might be related to scar tissue, or impingement of the iliopsoas (hip flexor) tendon against the prosthesis after hip replacement.
Pain in the hip flexor region at the front of the hip can also be referred from the low back (lumbar spine), the pelvic joints (Sacroiliac joints or SIJ’s), or the internal organs. Occasionally the problem can also be an infection in the iliopsoas bursa, although this is not common.
The poor hip flexors are regularly subjected to strong stretching techniques, deep massage, trigger point release (often very painful), acupuncture, needling or cortisone injections, foam roller massage, and all sorts of other torture inflicted with a whole range of tools!
And how much evidence is there that any of these things help?? … Zip! Zero! None!
In fact, not only are most of these things a waste of time and money for ‘hip flexor pain’, not to mention very painful, some may make it worse, and the pain might not even be related to the hip flexors!
Many people are stretching their hip flexors and placing high loads on the front of the hip unnecessarily, often aggravating their symptoms.
Hip flexor pain in sitting may be the result of how you are sitting, particularly if you are sitting for a long time, or it might not be hip flexor pain at all.
Do you use your chairback in sitting?
Or do you find yourself perching on the front edge of the chair?
Are you worried about ‘poor posture’?
Do you try to sit with ‘perfect posture’, completely upright?
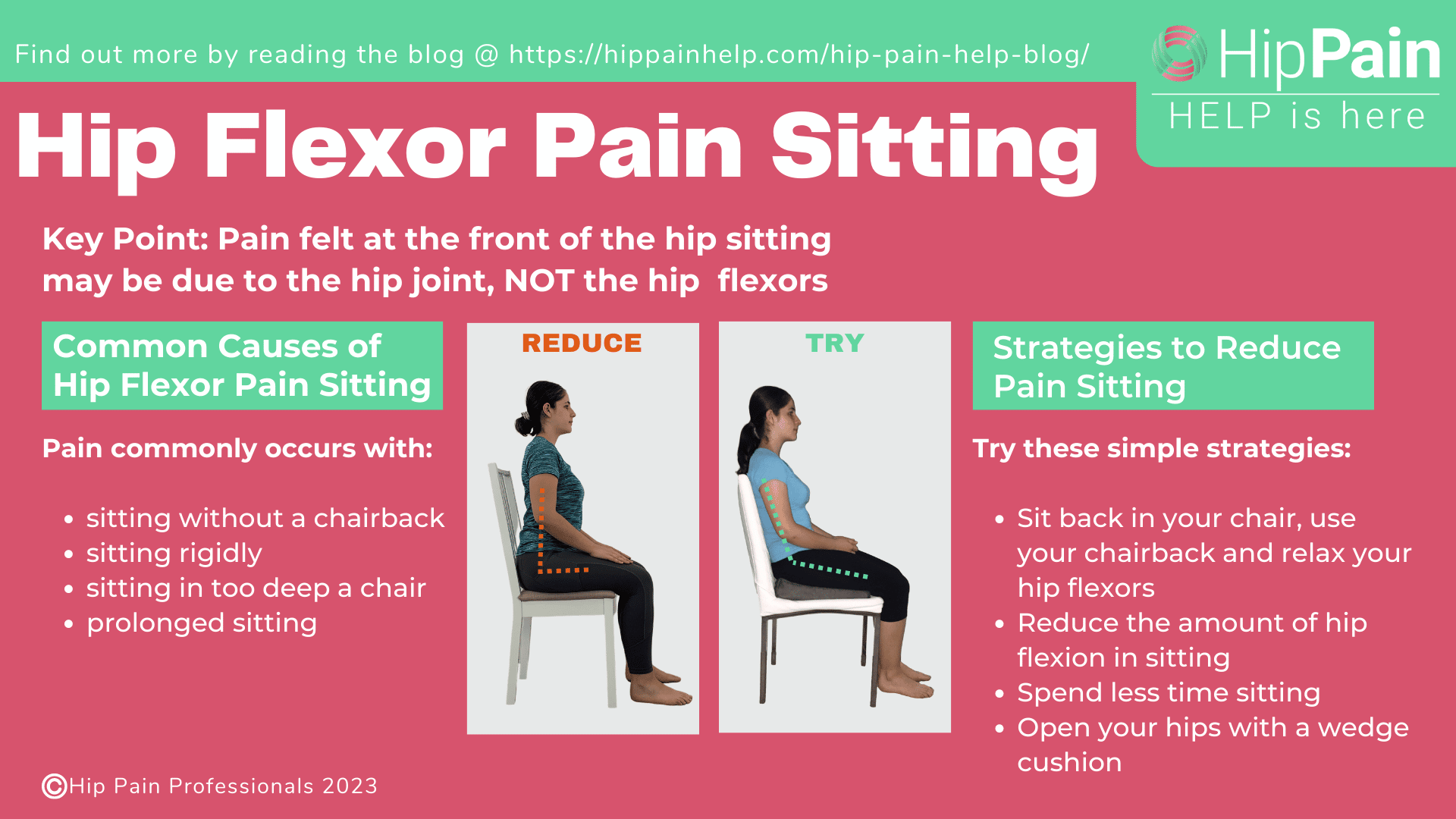
Trying to maintain these completely upright postures, without the support of the chairback, uses a whole lot of muscle activity – particularly in the lower back and the hip flexor muscles. This can get very fatiguing and for some may lead to hip flexor pain sitting and also lower back pain.
This pain may be related to the hip flexor muscles themselves, or the underlying joint structures. Irritable joint structures, for example, related to a labral tear, hip osteoarthritis, hip impingement, or hip dysplasia, may be irritated by hard-working hip flexors, if you are sitting in rigid, unsupported postures.
If you are more of a relaxed sitter who uses your chairback, but you still get hip flexor pain sitting, the pain might not be related to the hip flexors at all. Irritable joint structures just tend to become painful after prolonged sitting at 90° hip flexion or in deeper/lower chairs.
You might also experience hip flexor pain after sitting when rising to stand. If you have been working hard on these muscles during sitting, you might have pain trying to relax and lengthen them as you stand up. Or it can be the joint complaining as you re-load it.
Luckily, regardless of whether your hip flexor pain sitting is actually your hip flexors or your hip joint, the same sort of strategies will help to reduce pain in both.
Here are some great strategies for reducing hip flexor pain in sitting (and joint pain):
1. Sit back in your chair, use your chairback, and relax your hip flexors,
2. Reduce the amount of hip flexion in sitting, and
3. Spend less time sitting.
A great way to reduce tension in the iliopsoas muscles and back muscles is to make a point of moving your bottom to the back of the chair each time you sit down, relaxing onto the chair back. Avoid perching and leaning forward towards your desk. If your chair arms are stopping you from getting your chair under the table – remove them!
If you still have pain, you might need to open up those hips a little more. One simple strategy for reducing your front-of-hip pain sitting is to sit with your hips slightly higher than your knees. A posture wedge is a cheap, portable way to do this easily on all chairs you use, including when driving or travelling. Check out more about the wedge cushion by clicking HERE
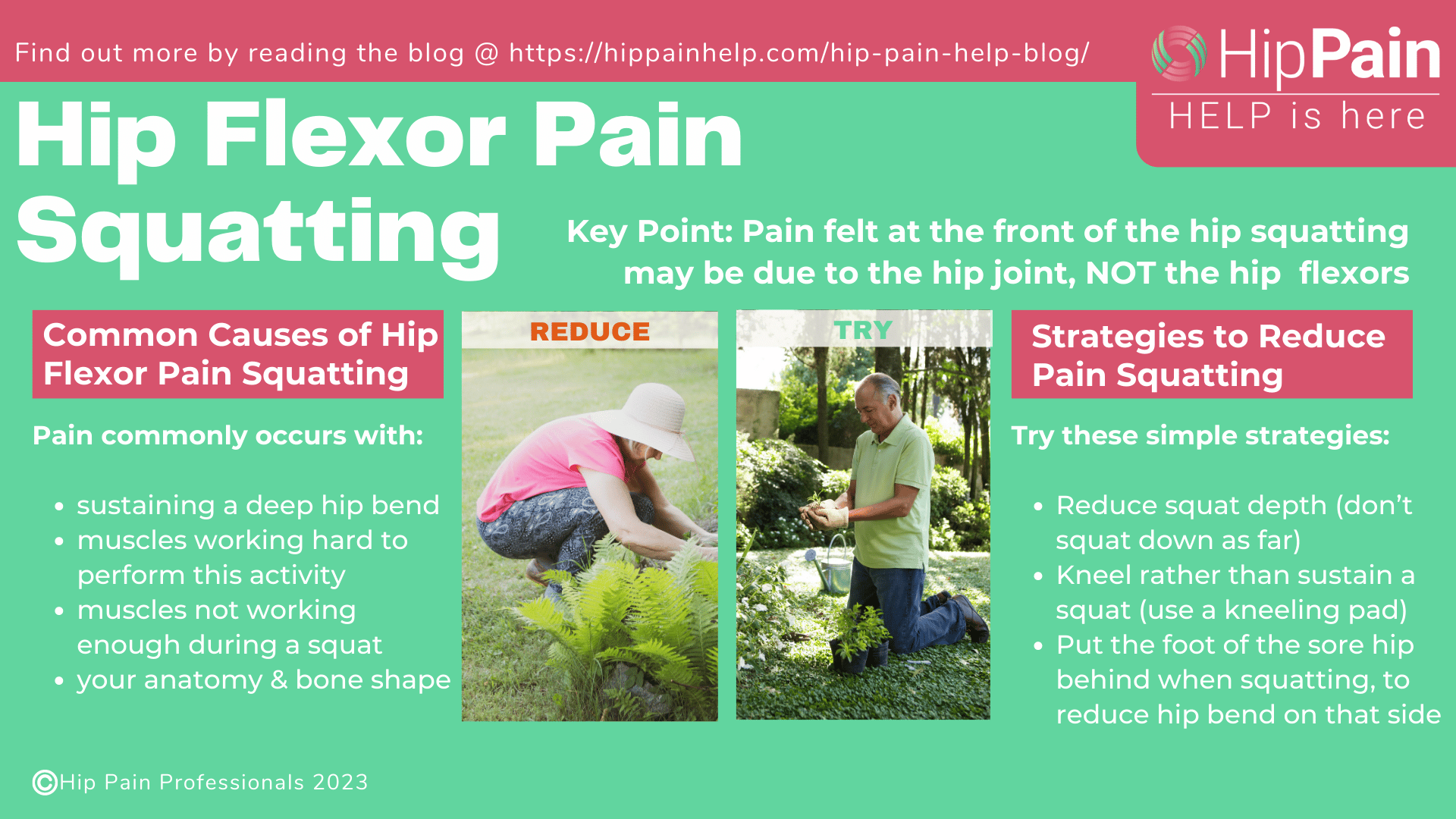
Squatting requires the hip to bend (hip flexion). Squatting lower requires a deeper hip bend at the bottom of your squat. Deep hip flexion can result in pain related to the hip flexors or the underlying joint.
It is possible that deep hip flexion may result in physical compression of irritable hip flexors at the front of the hip, but these muscles have also been shown to be working hard at the bottom of a squat.2
Why are the hip flexors working in a deep squat? This is a movement that the large gluteal and quadriceps muscles at the front of the thigh create and control. The hip flexors might be working to keep the body close to the thigh, helping to keep the hip bent at the bottom of the squat.
Researchers have also suggested that the deepest hip flexor muscles that join onto the hip capsule may have a special role here.2 In deep hip flexion, these muscles may provide support for the joint and help keep the capsule on tension as it becomes slack in a squat position. This will ensure the joint capsule does not get pinched in the front of the joint in a deep squat.
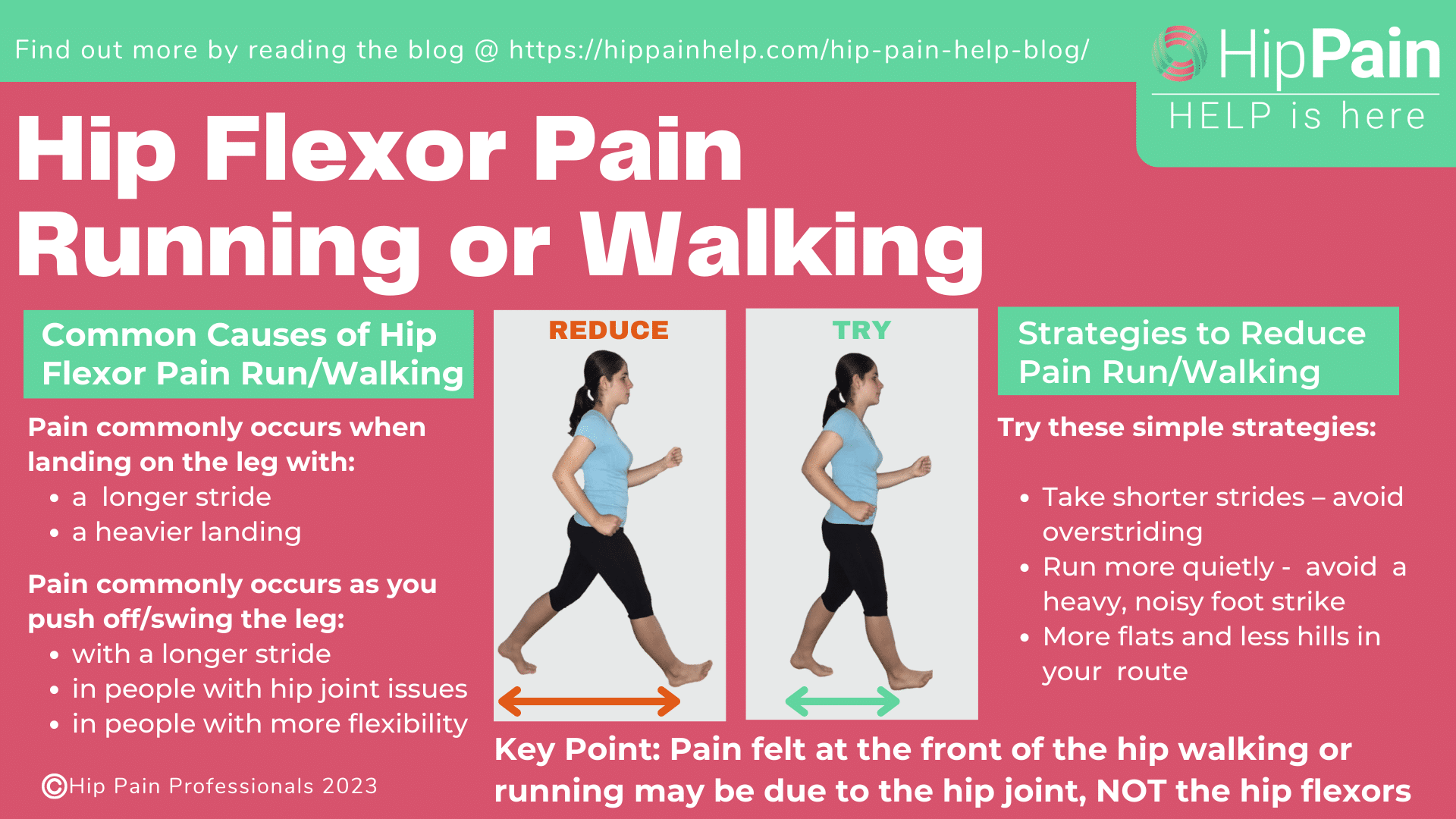
Hip flexor pain walking or running may occur either when your foot hits the ground, as you push off, or both.
Pain at the front of your hip as you land is less likely to be from the hip flexors. At this point, there are sudden ground reaction forces from hitting the ground. These travel up the leg and some of this force is absorbed in the hip. It is therefore more likely that pain felt at the front of the hip when your foot hits the ground is related to the hip joint – for example, the bone beneath the hip cartilage, or the hip labrum.
Walking and running styles that use long strides and heavy impact are likely to be more problematic.
Pain felt at push-off and in the early swing phase may well be linked to your hip flexors. At this point, the iliacus and psoas muscles have an important role in helping to control the hip joint – supporting the ball at the top of the femur, in the hip socket (acetabulum).
Long striding walking or running will not only lead to higher impact forces but increased forces at the front of the hip as you push off.
In people with particularly mobile hips, secondary to conditions such as hip dysplasia, hypermobility, or Ehlers-Danlos Syndrome, the hip flexors may have to work more than normal to control the high loads at push-off. In some people, this may result in pain over time.
Alternatively, it may be the hip joint and structures within the front part of the hip joint that are painful. This could be linked with FAIS (femoroacetabular impingement syndrome), hip osteoarthritis, or with hip labral tears.
Try one of these 3 simple strategies to reduce pain at the front of your hip from your hip flexors with running or walking:
You can read more about reducing hip pain walking and running by clicking HERE
Hip flexor pain cycling is most commonly felt if you have cleats and are pulling up hard, or at the top of the pedal stroke.
If you use cleats, the hip flexors help to pull the foot up to the top of the stroke, while you push down on the other side with the thigh and gluteal muscles. Focusing more on the upstroke will increase the load on the hip flexors.
Harder work, like riding uphill and sitting in the saddle might increase contribution from the flexors, particularly if you start to get tired in the quads muscles at the front of the thigh, you might start using more hip flexors.
None of this is problematic unless you do too much too quickly and push the hip flexors past their capacity. And particularly if you keep doing this without adequate recovery.
If your cycling action is more of a push than a pull, or if you don’t have cleats, then your front-of-hip pain cycling may be more about the hip joint position. At the top of the cycle action (12 o’clock position), when the knee is closest to the chest, the structures at the front of the hip joint are compressed and for some people, this may become painful.
Pain is more likely to occur related to hip conditions like FAIS (femoroacetabular impingement syndrome), hip osteoarthritis, or hip labral tears.
If your hip flexor pain is due to the pull-up, you may have to reduce your load:
1. Reduce your cycling distance,
2. Reduce your speed, or
3. Reduce the hills for a period of time, and
4. Increase recovery time to allow your hip flexors to recover.
This needs to be done in conjunction with a rehabilitation program to help strengthen the hip flexor muscles as well as the other muscles of the hip, pelvis, trunk, and leg. You may need to consult with a Hip Pain Professional, a physical therapist, or an exercise physiologist who understands hip pain specifically.
If your pain is more related to the position of your hip at the top of the cycle stroke, addressing your position on the bike will be key to your recovery. You need to open up the angle at the front of the hip so that the hip is not as bent.
Strategies to improve your hip joint related pain on the bike may include:
Getting a bike fit assessment may be extremely useful in this case. Some physiotherapists/physical therapists with an interest in hip pain also have a special interest in bike set ups. You can use our “Find a Professional” directory to see if there is a health professional near you that does both these things.
Pain at the front of the hip when walking up stairs is most likely to be felt when the foot is off the ground and your hip flexors are lifting the weight of the leg. Pain at the front of the hip when pushing through the foot might be more related to the hip joint or sometimes referred from the back or pelvic joints.
We’ve written a whole blog on hip pain when walking up stairs, so you can find loads of information there on hip flexor pain or other reasons for hip pain when walking up stairs. Click HERE to read this blog.
Pain in the front of the hip can be tricky to diagnose, understand and treat. We hope that this and other articles at hippainhelp.com help you better understand what your issues might be and how you can get started with some simple rehabilitation and self-treatment ideas.
We also hope we’ve dispelled some myths, which can often see people spending loads of time and money on strategies that have no evidence and are unlikely to be helpful in the longer term.
After following some of this advice, if your pain continues make sure you seek the help of a health professional who better understands hips and hip pain, and check into your treatment options. The best first step may be a physical therapist, or in the case where you may have already done this, an orthopaedic surgeon. A good trial of physical therapy should always be undertaken before a visit to a surgeon.
You can check out our global network of health professionals, who know hip and pelvic pain, by clicking HERE
This blog was written by Dr. Alison Grimaldi, with contribution from one of our Hip Pain Professionals, Kirsty McNab, experienced physiotherapist.
Dr. Alison Grimaldi is a globally recognised expert physiotherapist, researcher, and educator, who has over 30 years professional clinical experience helping patients recover from a wide range of hip and pelvic conditions.

Dr. Alison Grimaldi BPhty, MPhty(Sports), PhD, FACP
Dr Grimaldi has completed Bachelor of Physiotherapy, Master of Physiotherapy and Doctor of Philosophy (Physiotherapy) degrees. She is a fellow of the Australian College of Physiotherapists, Practice Principal of PhysioTec Physiotherapy, an Australian Sports Physiotherapist , an Adjunct Senior Research Fellow at the University of Queensland, as well as an author and global educator. Her passion is helping people with hip pain, and educating other health professionals around how to help more people with hip pain.